


Abstract
IgA nephropathy (IgAN) is a fairly common association with alcoholic liver disease. However, IgA vasculitis (IgAV) is quite an uncommon association with alcoholic liver cirrhosis and only a handful of cases have been reported in literature. Secondary IgAN usually presents in a docile manner, progressing slowly in about 5-25 years. It is usually responsive to steroid therapy, very rarely progressing to End-Stage Renal Disease.
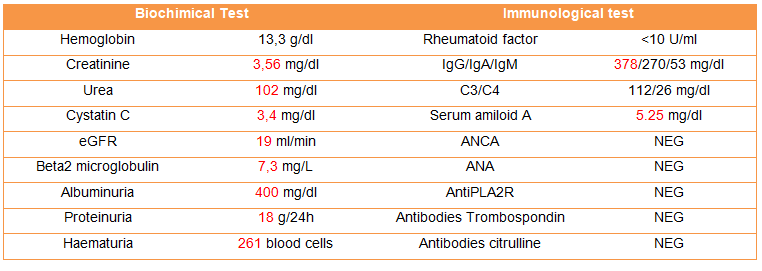
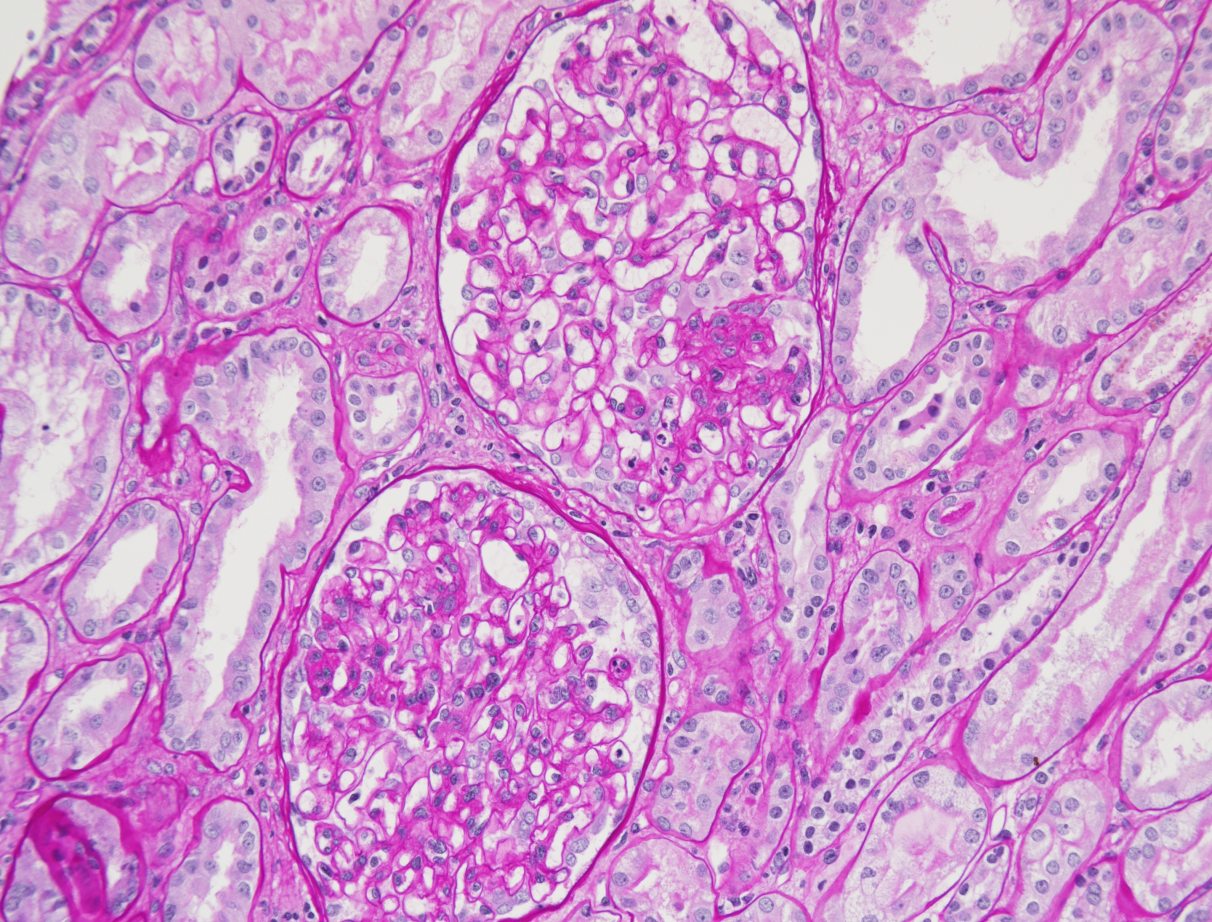
Here, we present a man in his late 50s, a known hypertensive and alcohol related liver-cirrhotic, who presented to our hospital with rash and rapidly progressive renal failure (RPRF). He was diagnosed with IgA nephritis with IgA vasculitis (IgAVN). His diagnosis was confirmed with skin and renal biopsy.
He was started on renal replacement therapy for his renal failure and began oral steroid therapy. After administration of steroid therapy for 6 months, the patient recovered and was dialysis independent with stable renal parameters.
Keywords: IgA nephropathy, Alcoholic Liver disease, rapidly progressive glomerulonephritis, IgA vasculitis



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}