

Abstract
Giuseppe Moscati occupies a distinctive place in Italian medicine of the early twentieth century, a period marked by the rapid development of experimental physiology, clinical chemistry, and the first systematic laboratory diagnostics. Although he is often remembered today primarily for his spiritual legacy, Moscati was deeply rooted in scientific research: he regularly used urinalysis to guide clinical decisions, showed early interest in ureogenesis, and referred in his prescriptions to conditions such as “oxalic diathesis”. For these reasons, his work continues to inspire modern nephrologists.
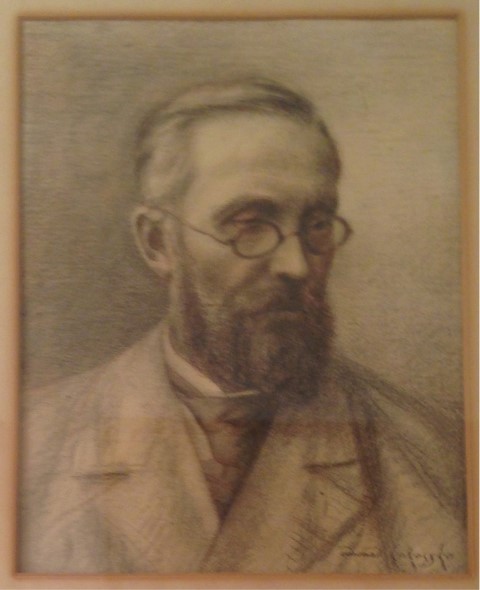
Born in Benevento in 1880 and educated in Naples, he graduated in 1903 with a thesis on hepatic ureogenesis. He quickly entered hospital work and scientific research, training in the laboratories of Albini, Malerba, and Bottazzi. After his early appointments at the Ospedali Riuniti, in 1919 he became chief physician of the Ospedale degli Incurabili and later professor of Physiological Chemistry and Clinical Medicine at the Royal University of Naples. Beatified in 1975 and canonized in 1987, Moscati has more recently been recognized for his scientific contributions; several studies describe him as a pioneer of Italian biochemistry and early diabetes research. His investigations on metabolism, placental function, glycogen dynamics, and endocrine physiology were discussed internationally and cited in major scientific journals.
The unpublished prescription dated 24 February 1923, preserved in a private collection, provides concrete insight into his clinical method. Faced with a patient suffering from renal calculi with a luetic background, Moscati constructs a stepwise therapeutic plan beginning with laboratory observation, followed by dietary measures and symptomatic treatments, and resorting to more aggressive therapy – such as mercurial injections – only if preliminary conditions were favorable. His instructions illustrate a natural integration of dietetics, phytotherapy, pharmacology, and clinical caution. The direct and practical tone reveals a physician close to the patient, attentive to daily life and vulnerability. This prescription thus becomes a valuable document that shows the real Moscati: a rigorous scientist, a meticulous clinician, and a man profoundly dedicated to care.
Keywords: history, urine analysis, urine sediment, kidney stones








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}