


Abstract
Background: In order to minimize the risk of leakage and displacement, international guidelines recommend that catheter insertion should be performed at least 2 weeks before beginning CAPD. However, the optimal duration of the break-in period is not defined yet.
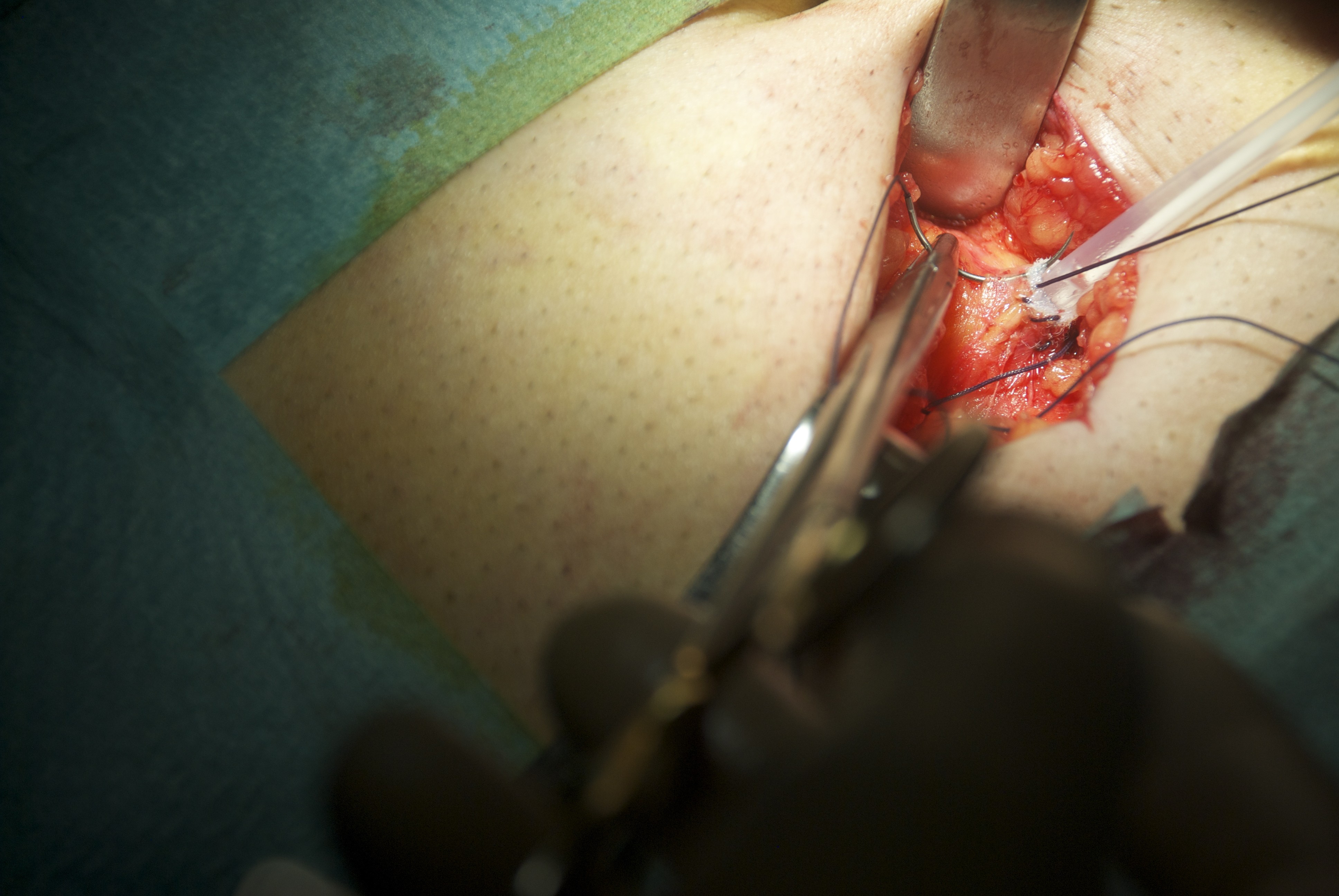
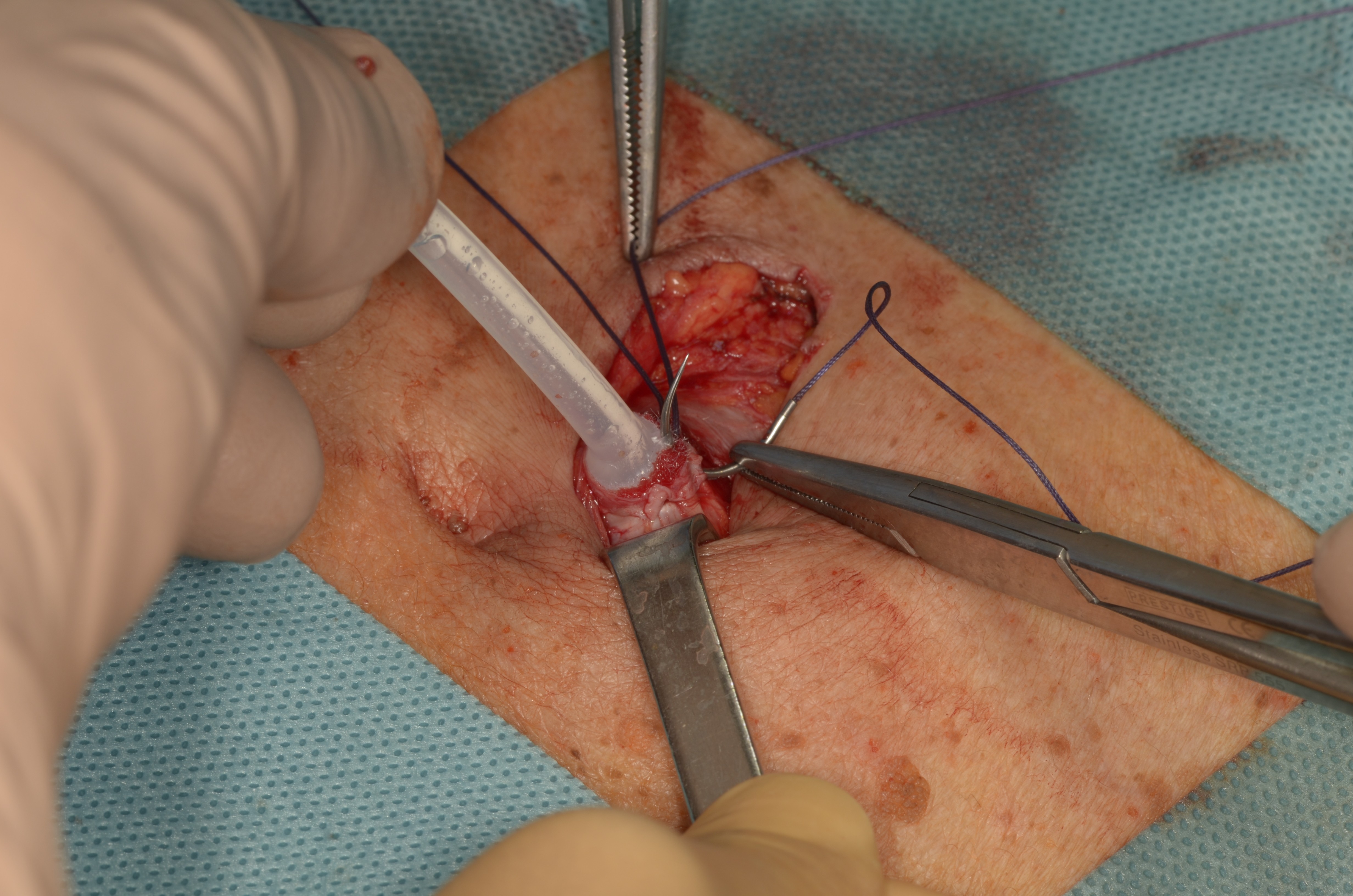
Methods: From January 2011 to December 2018, 135 PD catheter insertions in 125 patients (90 men and 35 women, mean age 62,02 ± 16,7) were performed in our centre with the double purse-string technique. Seventy-seven straight double-cuffed Tenckhoff catheter were implanted semi-surgically on midline under umbilicus by a trocar and 58 were surgically implanted through rectus muscle. In all patients CAPD was started within 24 hours from catheter placement, without a break-in procedure. We recorded all mechanical and infective catheter-related complications during the 3 first months after initiation of CAPD and the catheter survival rates.
Results: During the first 3 months the overall incidence of peri-catheter leakages, catheter dislocations, peritonitis and exit-site infections was 2,96% (4/135), 1,48% (2/135), 10.3% (14/135) and 2.96% (4/135), respectively. No bleeding events, bowel perforations or hernia formations were reported. The catheter survival censored for deaths, kidney transplant, loss of ultrafiltration and inability was 74,7% at 48 months. There was no difference in the incidence of any mechanical or infectious complications and catheter survival between the semi-surgical and the surgical groups.
Conclusions: Double purse-string technique allows an immediate start of CAPD both with semi-surgical and surgical catheter implantation. This technique is a safe and feasible approach in all patients who refer to peritoneal dialysis.
Keywords: continuous ambulatory peritoneal dialysis, CAPD, peritoneal catheter, break-in time, infective catheter-related complications, double purse-string technique

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}