Abstract
Peritoneal dialysis has shown to reduce days of hospitalization, NYHA functional class and to improve slightly left ventricular ejection fraction in heart failure patients. For the first time, the nationwide 2024 Census of the Peritoneal Dialysis Project Group of the Italian Society of Nephrology is able to analyze and to confront heart failure patients treated by peritoneal dialysis to a time-matched cohort of chronic kidney disease patients under peritoneal dialysis.
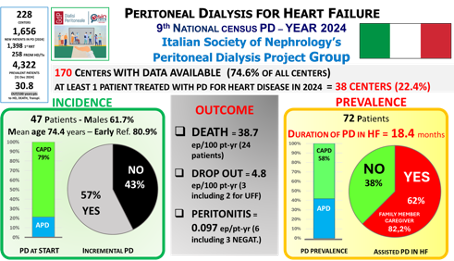
The census data of 170 Italian dialysis centers are presented. 1063 patients started peritoneal dialysis for kidney disease whereas 47 patients for heart failure, resulting in a prevalence of 3371 kidney disease patients and 72 heart failure patients in 2024. Heart failure patients presented higher age and male prevalence. CAPD was mainly used as dialysis start modality in heart failure patients (78.7%) with incremental dialysis prescription more often applied and assisted dialysis more often needed.
Mean duration of peritoneal dialysis was 31.3 months in kidney disease patients, whereas 17.6 months in heart failure patients, mainly due to a 4-fold increased risk of death. The peritonitis risk was lower in heart failure patients with 0.097 episodes / patient-year compared to 0.166 episodes / patient-year in kidney disease patients.
The census results confirm that peritoneal dialysis for heart failure is a feasible time-limited therapeutic opportunity for a known high-risk population of mostly elderly, male and frail patients requiring assisted dialysis.
KEYWORDS: peritoneal dialysis, chronic kidney disease, heart failure, survival, peritonitis, census