Abstract
Assisted peritoneal dialysis (PD) is an important option for frail patients with advanced age, comorbidities, and reduced autonomy who face barriers to self-managed home dialysis. This study evaluates the current use of assisted PD in Italy using data from the 2024 Italian Peritoneal Dialysis Census and compares findings with previous surveys conducted since 2008.
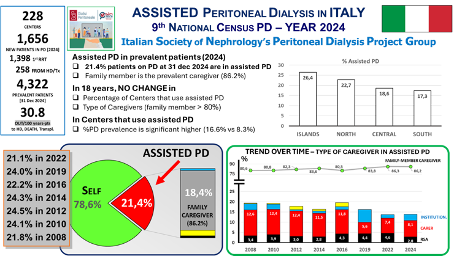
Data were collected from 228 dialysis centers, with 221 centers providing information on assisted PD, covering 4,229 prevalent PD patients. Assisted PD was reported in 904 patients (21.4%). Family members were the main caregivers (86.2%), followed by paid caregivers (8.1%), institutional staff (2.9%), and nursing home personnel (2.8%). Over time, the proportion of assisted PD remained stable between 21% and 25%, with no significant change in caregiver distribution.
Centers applying assisted PD were larger, had higher PD prevalence, and managed more PD patients compared with centers not using assisted PD. Geographic variability was observed, with the highest prevalence in island regions. Only a small proportion of patients in nursing homes were treated with PD compared to hemodialysis, highlighting organizational and staffing barriers.
These findings show that assisted PD in Italy has remained stable over the past two decades and is predominantly based on family caregiving, unlike Northern European countries where professional home care predominates. The limited use of institutional and nursing home support suggests unmet needs and potential areas for improvement. Economic incentives, regional support programs, and telemedicine may help expand assisted PD access and promote home-based dialysis in frail populations.
KEYWORDS: peritoneal dialysis, assisted peritoneal dialysis, caregiver