

Abstract
Introduction. Incremental peritoneal dialysis (Incr-PD) is a strategy to start PD when residual renal function is preserved.
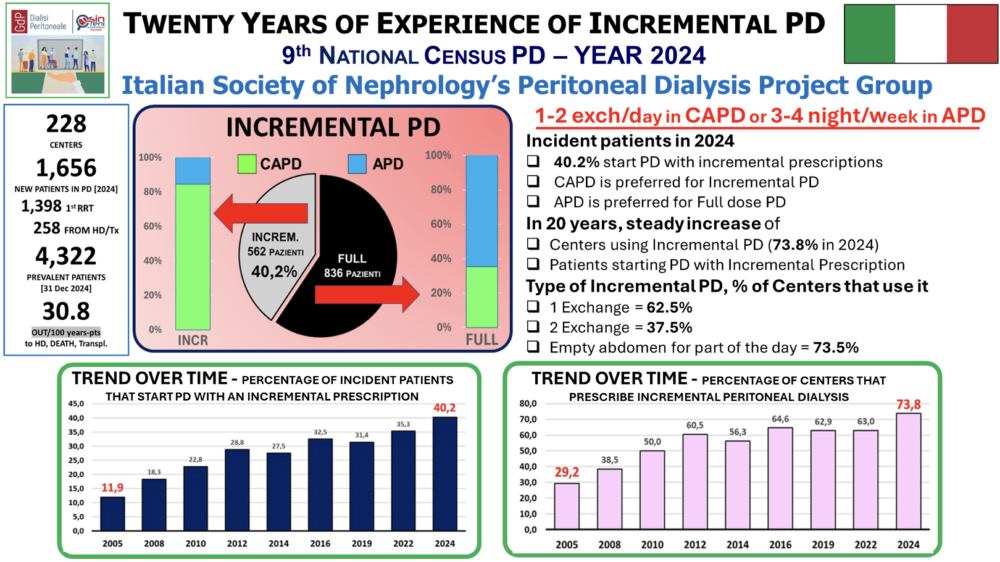
Methods. We describe the Incr-PD practice across the last 20 years based on the 9th Italian PD Census utilizing a standardized definition of Incr-PD for both CAPD and APD (≤2 exchanges/day, ≤4 sessions/week).
Results. In 2024, 1398 patients started PD, 40.2% on Incr-PD. 73.8% of the dialysis centers used Incr-PD. Incr-PD increased from 11.9% in 2010 to 40.2% in 2024. This is due to both the increase in the number of centers which started to use it (29.2% in 2005 to 73.8% in 2024) and in the number of patients treated with this modality in centers already confident with this modality (33.4% in 2005 vs 50.9% in 2024). Most of Incr-PD patients started with CAPD (84.5%) while APD was the preferred modality when full-PD is prescribed as first PD modality (64.7%). Regarding incremental CAPD, 62.5% of physicians start with one exchange, while 37.4% use two. In the latter case, only 26.2% prescribe two continuous exchanges with “the abdomen always full”. Incr-PD centers have higher incidence (21.7% vs 15.1%, p < 0.01) and prevalence (16.9% vs 12%, p < 0.01) of PD patients compared with those not using it. Conclusions. The trend confirms the success of Incr-PD, mostly in the form of CAPD. The increased Nephrologist’s confidence with Incr-PD allowed the expansion of this PD modality which is the mainstay of dialysis personalization.
KEYWORDS: peritoneal dialysis, incremental peritoneal dialysis, census report